Background Information
The morphology of the hip joint from birth to adolescence is a progressive process influenced by load and an individual’s genetic composition (Hogervorst, Boumer, De Boer, & de Vos, 2011) . Variations in normal morphology of the proximal femur and acetabulum in addition to excessive loads can lay the foundations for chondral and labral injuries and subsequent early degenerative changes (Giordano, 2014). Evidence has suggested that participation in impact sports encouraging heavy, repetitive loading prior to physeal closure can result in an increased prevalence of overuse enthesopathies, traumatic avulsions or the development of cam lesions in children and adolescents (Siebenrock et al., 2011).
As physiotherapists, it is our responsibility to perform thorough assessments on children and adolescents presenting with hip pain to not only exclude serious pathology but also discuss appropriate load management (e.g suitable recreational activities) and to prevent further long term complications (Giordano, 2014).
The first two minutes of this video is a basic review of the anatomy of the hip in an infant or adolescent.
Age Related Hip Presentations
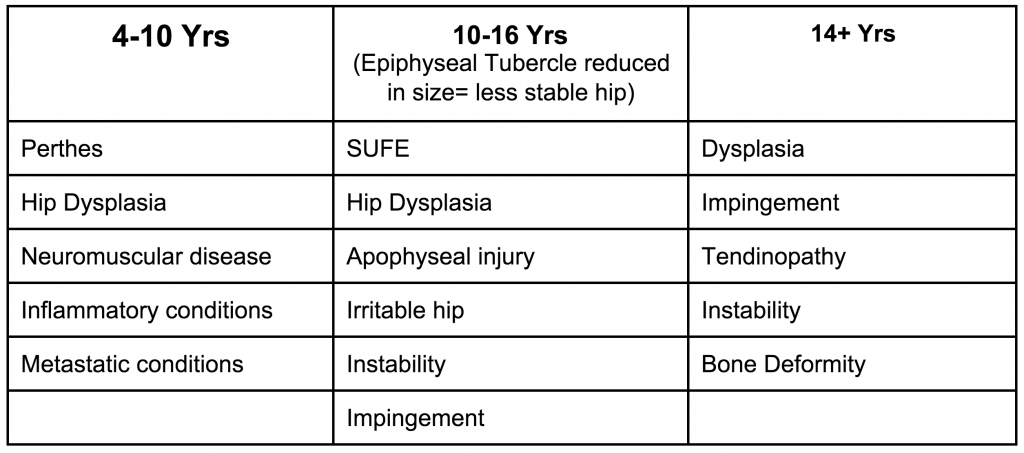 (Rath, 2014)
(Rath, 2014)
Subjective Assessment
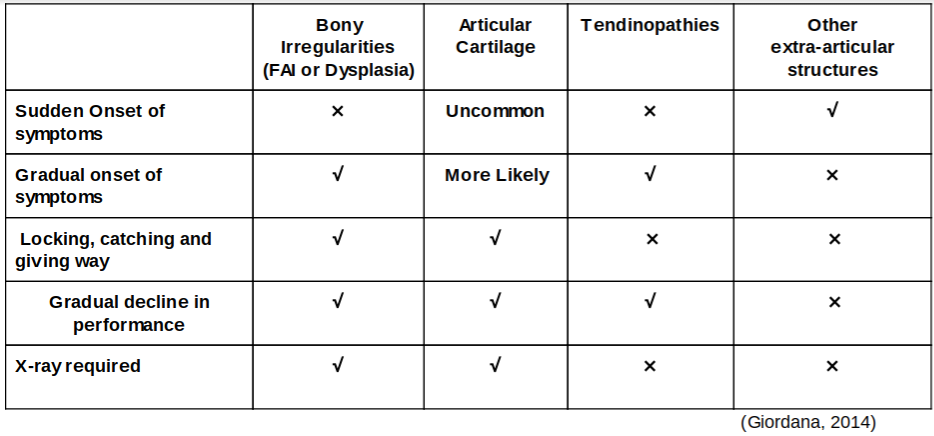
When assessing an infant or adolescent hip it is important to establish the behaviour of the symptoms to differentiate an acute injury from conditions related to altered bony morphology e.g dysplasia or Femoral Acetabular Impingement (FAI) (Martin, & Palmer, 2013). Pain from a single loading episode followed by difficulty weight bearing and restricted range of motion typically indicate an acute injury involving the physis and soft tissues rather than deeper intra-articular structures. In contrast, children with potential bony morphology, articular cartilage injury or tendon pathologies report a gradual onset of pain, locking/catching or giving way and a gradual deterioration in athletic performance (Giordano, 2014).
Children with FAI or instability will report episodes of locking, catching, grinding or giving way in their hip. Differential diagnosis of these conditions is difficult due to the similar signs and symptoms reported (Kappe et al., 2012). Clinicians need to establish the behaviour of the child’s symptoms in addition to identifying provocative positions. For example, a child reporting pain when the hip is internally rotated and flexed, followed by giving way, is more likely to have a muscle inhibition as a consequence of impingement. This is in contrast to a patient with instability, who may report the sensation of their hip moving out of the socket in the absence of pain (Boykin et al., 2011).
Children exhibiting a gradual onset of symptoms should be referred for radiological evaluation as patient history alone cannot determine a definitive diagnosis or the severity of morphological abnormality. It is recommended that a A-P bilateral hip X-ray in standing and unilateral X-ray of the symptomatic side be performed (Kappe et., 2012)
Children presenting with pain that is diurnal, not reproducible with physical activity and that is unpredictable in nature may indicate the presence of a systemic condition and require immediate referral for further investigations (Giordano, 2014).
Stay Tuned
Our next blog post will focus on how to assess hip X-rays.
If you have a paediatric or adolescent patient presenting with hip pain that you would like to refer to Little Humans Physio for a consultation, you can contact us or make an online referral.
Reference List
Giordana, B. (2014). Assessment and treatment of hip pain in the adolescent athlete. Pediatric Clinics of North America, 61(6), 1137-1154.
Hogervost, T., Bouma, H., de Boer, S., & de Vos, J. (2011). Human hip impingement morphology: an evolutionary explanation. Journal of Bone and Joint Surgery, 93(6), 769-776.
Martin, H., & Palmer I. (2013). History and physical examination of the hip: The basics. Current Review Musculoskeletal Medicine, 6(3), 219–25.
Roth, L. (2014). The developing hip of the adolescent athlete. Adolescents in Sport Symposium.
Sienbenrock, K., Ferner, F., Noble, P., Santore, R., Werlen, S., & Mamisch, C. (2011). The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clinical Orthopaedics and Related Research, 469(11), 3229-3240.